Classification
Degrees of Hazard
The classification of lasers is based on the potential hazard they present to people exposed to them, with the higher number denoting greater potential hazard. The numbers have nothing to do with any progression of technical development. All classes have been around and used since the introduction of classification.
Classes 3B and 4 lasers are distinguished by power levels with Class 3B being those up to 500mW and Class 4 being greater than 500mW. Both are powerful enough to present potential hazard: Class 3B mainly to the eye and Class 4 to skin and tissue as well as the eye. Hence the common medical use of Class 4 lasers for surgical purposes, where targeted tissue destruction is the objective. Class 4 also present a potential hazard with respect to reflections off a range of surfaces but with Class 3B this is limited to mirror reflections when the beam is highly collimated.
Omega produces Class 3B laser systems which are completely safe so long as the protective eyewear is worn.

"... although the specific boundaries of rule of reciprocity (i.e. that high power for a shorter time is equivalent to low power for a longer time) are not yet firmly defined, it is known that treatments of much higher powers can require times too short for the body to react to, and vice versa."
Faster Can Mean Ineffective
Limited Reciprocity
The law of reciprocity in the context of laser therapy refers to the theoretical idea that the same physiological effect can be achieved with a particular amount of energy whether using a higher power for a shorter time or a lower power for a longer time. This 'law' however, does not apply beyond a close range of variation. If the power density is too low, no matter how long the treatment time, the desired effect is unlikely to be achieved and if the power density is too high the cells have inadequate time to react to the irradiation also rendering the treatment ineffective.
The maximum power of Class 3B lasers, permitting fastest speed of delivery of effective doses, tends not to be utilised because that would already exceed the speed at which the cells can react, so why a laser capable of even faster delivery would be preferable is unclear. Faster delivery would at least require evidence that effectiveness is maintained, let alone improved.
Stronger Doesn't Equal Better
Therapeutic Energy Window
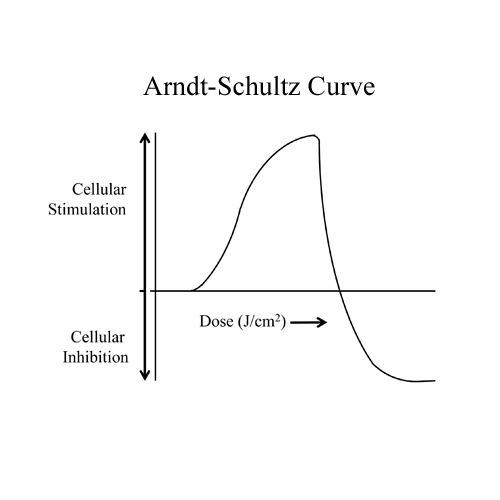
The physiological responses to light have been shown to correlate with the Arndt-Schultz curve whereby the stimulatory effect increases with energy input up to a certain level and then as the energy increases further the effect diminishes until it becomes inhibitory.
Over the years, protocols for photobiomodulation have been refined with the aim of excluding overtreatment except where inhibition is intended. Simply adding in more power is not a predictor of better effect. In fact, this presents a risk of overtreatment possibly resulting in inhibition of pain without stimulation of the healing process leading to potential overuse whilst compromised and so further injury.
..."Transcranial application of 808 nm wavelength light penetrated the scalp, skull, meninges, and brain to a depth of approximately 40 mm with an effective attenuation coefficient for the system of 2.22 cm−1. No differences were observed in the results between the Pulsed Wave and Continuous Wave laser light..."
Penetration of Tissue
Wavelength is Key
It has been commonplace for Class 4 laser promoters to claim that the high-power of their lasers enables deeper treatment (although most are now qualifying such claims in their written materials). The research however all concurs that wavelength, not power, is the key factor for depth of tissue penetration.
Deepest penetration has consistently been shown to be achieved by light in the early 800nm near infra-red range which suffers less scattering and irrelevant absorption as it passes through the tissue. The 820nm wavelength has also been shown as a good 'all-rounder' with respect to stimulating response in a range of cell types, which is not the case for all wavelengths. An 820nm wavelength delivered by a Class 3B laser such as Omega's will penetrate deeper than a 980nm wavelength regardless of laser class.
Research has also shown tertiary and systemic effects occurring distal to the site of primary absorption of photons and of course, for many applications, deep tissue penetration is not an issue and care must be taken that relevant wavelengths are used and that the required energy is delivered slowly enough to have best effect.
Super-Pulsing
Back to Speed and Reaction Time
Super-pulsing is variously claimed to be a new development, to facilitate deeper treatment and to deliver greater density of energy to target cells.
In fact, super-pulsing is not new - Omega has offered a super-pulsed probe for over 20 years; it has only a secondary effect on depth of penetration through tissue which is overwhelmingly determined by wavelength; and although theoretically it might enable quicker delivery of energy doses to the deepest target cells, in vivo evidence is scant and mixed, and clinical benefit questionable.
As discussed already, delivering energy too quickly negatively affects efficacy, so if super-pulsing is being used to deliver more energy to deep target cells more quickly then it can't be assumed that such a different speed of delivery remains effective, let alone an improvement, without evidence.
Also, super-pulsed lasers tend to be named according to their peak power possible, but they emit in extremely quick pulses and only emit during those brief pulses, so depending upon their set-up, and particularly how low the duty cycle is (i.e. % of time actually emitting), the actual energy delivered can be just a tiny fraction of that possible from the headline peak power and possibly below that of a pulsed diode Class 3B laser.
Are Doses Actually Different?
Key Parameters Missing
Research tells us that the correct energy density 'dose' (usually measured at skin surface for easy comparison) is critical for effective treatment and is a key parameter in terms of comparing studies. However, this parameter is interestingly omitted by Class 4 manufacturers from their publicity and study reports.
Analysis of one Class 4 laser study which gave enough other parameters to calculate this measure, showed it to be not only within 3B low level laser capabilities but actually lower than the recommended photobiomodulation energy 'dose' usually delivered with the Class 3Bs.
It is difficult to see why such key parameters would be omitted other than to obscure energy doses, and similarly difficult to see why one might want to obscure energy doses unless comparison would prove inconvenient. This apparent obfuscation combined with common recommendations of non-contact techniques, which can hugely reduce energy delivered into the tissue, leaves open the question as to whether the energy delivered into tissue by Class 4 lasers is any greater than that delivered by Class 3B lasers at all.
If the energy is greater or is being delivered more quickly, then this requires evidence that treatment remains effective. If not, then why use such an over-engineered tool for the job?
Why Introduce Class 4 Lasers if Class 3B Lasers Work?
Clinical or Commercial Motivation?
PhotoBioModulation has always suffered commercially from being an open research field. Patents are not practicably enforceable since appropriately delivered laser light of appropriate wavelengths works, whatever the equipment, and the action is generic. This has constrained marketing investment and contributed to PBM's difficulties in competing with the dominance of big pharma despite its effectiveness and research base.
To make big profits in PBM equipment manufacture, one would need to at least claim that one's equipment was somehow substantively different from other equipment on the market and that it had exclusively better results. With all the major manufacturers in the field having sensibly converged upon producing forms of the optimal Class 3B lasers over the years, using a different class of laser to deliver the treatments would provide the opportunity to claim difference. Setting a reassuringly high price and loudly asserting superiority might even overcome the lack of comparative research required to claim improved results and there's always the 3B research base for support of effectiveness for PBM in general.
Class 4 lasers might prove to be as effective for photobiomodulation as the safer, less expensive, proven Class 3B lasers, but assertions of their superiority are completely unsupported.

Contact us
Contact Omega to discuss the application of laser in your practice.
Call +44 (0) 1787 477551 or email info@omegalaser.co.uk
